
Ultrasound-Guided Vascular Access: Where It Adds Value
Founder & Clinical Director, Ultrascan Technologies
March 9, 2026 - 8 min read
Vascular access failure is one of the most common procedural complications in clinical medicine. Failed peripheral IV attempts cause patient distress, delay treatment, and consume nursing and medical time disproportionate to their apparent simplicity. For central venous catheters, failed attempts carry the added risk of pneumothorax, arterial puncture, and haematoma formation. Ultrasound guidance addresses these problems with a robust evidence base and increasingly accessible technology.
This article reviews the evidence for ultrasound-guided vascular access across peripheral and central applications, summarises key guideline recommendations, and discusses how handheld ultrasound devices fit the procedural workflow.
Peripheral Intravenous Access
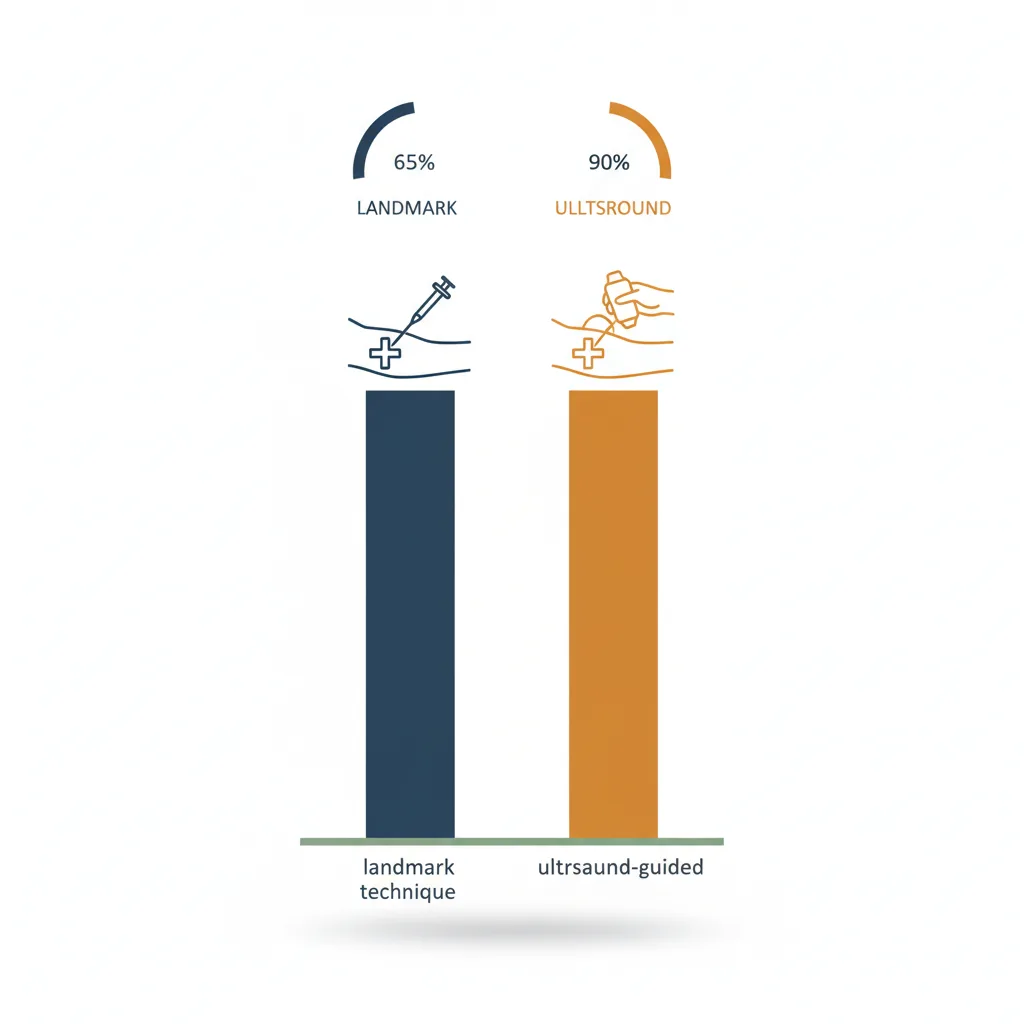
Standard peripheral IV placement by palpation and visual assessment fails at clinically significant rates in specific patient populations: the obese, the oedematous, patients with IV drug use history, those who have received multiple previous IV placements, and critically ill patients with vasoconstriction. In these "difficult access" patients, ultrasound guidance improves first-attempt success rates substantially.
A systematic review in the Annals of Emergency Medicine found that ultrasound-guided peripheral IV placement in difficult-access patients improved first-attempt success rates from approximately 33% (landmark technique) to over 80% (ultrasound-guided), with significant reductions in total cannulation time and the number of attempts per patient.
The antecubital fossa (basilic and cephalic veins) and the forearm are the preferred sites for ultrasound-guided peripheral access. The linear probe provides clear visualisation of veins as thin-walled, compressible anechoic structures. Needle tip visualisation in the short-axis (out-of-plane) approach is the most commonly taught technique for IV placement, though in-plane long-axis scanning allows continuous needle shaft tracking.
Central Venous Access: Internal Jugular
The internal jugular (IJ) vein is the most commonly cannulated central venous site, and ultrasound guidance for IJ access has the strongest evidence base of any central line application. The IJ lies lateral to the carotid artery in most patients, but significant anatomical variation is common - the vein may be anterior, medial, or even absent on one side. Ultrasound eliminates the guesswork.
The National Institute for Health and Care Excellence (NICE) in the UK recommends 2D ultrasound guidance as the preferred method for elective central venous catheter insertion in the IJ. Their technology appraisal TA49 on ultrasound-guided central venous catheter placement found that routine use of ultrasound guidance would prevent approximately 2,000 complications per year in the NHS and was cost-effective when device costs were considered.
In practice: place the linear probe transversely over the IJ at the level of the cricoid cartilage. The IJ appears as a large, thin-walled, easily compressible oval structure lateral to the pulsating, round carotid artery. Confirm the vein collapses with probe pressure - arteries do not. Needle entry in the short-axis (out-of-plane) view with continuous probe repositioning to track the needle tip is the standard technique.
Central Venous Access: Subclavian and Axillary
The subclavian vein approach has historically been associated with the lowest infection rates for central venous catheters, at the cost of a higher pneumothorax risk from traditional landmark technique. Ultrasound-guided infraclavicular subclavian (or axillary vein) access moves the puncture site laterally, where the vein is more accessible to imaging, the lung is further from the needle path, and the technique is genuinely safer.
The axillary vein is visualised at the level of the first rib with the probe placed infraclavicularly. The vein sits medial to the axillary artery and lateral to the first rib. In-plane (long-axis) needle visualisation is the preferred technique here, as you can watch the needle travel the full distance to the vessel wall before penetrating it.
Central Venous Access: Femoral
Femoral central access is reserved for situations where upper body sites are inaccessible or contraindicated. The femoral vein lies medial to the femoral artery in the femoral triangle. Ultrasound confirms the vein is patent (important in patients with prior femoral procedures or DVT), identifies anatomical variation, and reduces the risk of inadvertent arterial puncture.
Arterial Line Placement
Arterial line placement by palpation fails at rates up to 25% on the first attempt in intensive care patients, particularly those who are hypotensive or who have vasopressor-induced vasoconstriction. The radial artery typically has a diameter of only 2-3 mm, making ultrasound guidance particularly valuable in patients with reduced pulse pressure.
Short-axis visualisation of the radial artery at the wrist shows the artery as a pulsating, non-compressible circular structure. Dynamic needle tip tracking during puncture significantly improves first-attempt success. Evidence from ICU studies suggests ultrasound guidance reduces radial arterial line first-attempt failure by approximately 50% in haemodynamically unstable patients.
First-Pass Success Rates: The Numbers
A comprehensive systematic review published in Critical Care Medicine summarised the evidence across central and peripheral vascular access applications and reported:
- IJ central line: first-pass success improved from approximately 74% (landmark) to 94% (ultrasound)
- Arterial line placement: first-pass success improved from approximately 60% to 87% in critical care settings
- Overall complication rate reductions of 57% for central access with ultrasound guidance
Cost-Effectiveness
The cost-effectiveness of ultrasound guidance for vascular access is well established. The device cost is offset by reductions in complication treatment costs (pneumothorax drainage, arterial haematoma management, infection-related hospitalisation extension) and by reduced nursing and physician time on failed access attempts. A conservative estimate suggests that in a facility performing more than 200 central lines per year, an ultrasound device for vascular access guidance pays for itself within one year through avoided complications.
Choosing the Right Device for Vascular Access
For vascular access guidance, a high-frequency linear probe is the primary requirement. The linear array provides the image resolution needed to visualise small peripheral veins and distinguish the radial artery at the wrist. The Ultrascan US-PL includes a high-frequency linear element suitable for all standard vascular access applications. For dedicated vein-finding in nursing and emergency department workflows, the Ultrascan VF-10 vein finder provides a more portable, single-purpose solution for peripheral IV access in difficult patients.
To discuss which device best matches your procedural volume and setting, visit the Ultrascan contact page or review the full range of procedural ultrasound devices.
Visual Summary
Key concepts from this article at a glance.
Related Products
Related Articles

Bedside Cardiac Ultrasound: What Handheld Can and Cannot Tell You
Realistic expectations for focused cardiac ultrasound with handheld devices.

Ultrasound-Guided Regional Anaesthesia: Why Visualization Matters
The case for ultrasound guidance in nerve blocks and regional anaesthesia techniques.