
Practical Guide to FAST and eFAST with Handheld Ultrasound
Founder & Clinical Director, Ultrascan Technologies
March 11, 2026 - 10 min read
The Focused Assessment with Sonography for Trauma (FAST) exam is one of the highest-yield applications in emergency medicine. Performed correctly, it answers a critical question in under three minutes: is there free fluid in the abdomen or blood around the heart? The extended version, eFAST, adds bilateral pleural assessment for pneumothorax. With a handheld wireless probe, this exam can be initiated in the ambulance bay, the resuscitation room, or any clinical space where a trauma patient arrives.
This guide covers the protocol step by step, with attention to probe selection, patient positioning, common pitfalls, and when a positive FAST should prompt immediate escalation versus CT.
Indications: When to Perform FAST
FAST is indicated in any patient with a mechanism of injury that could cause intra-abdominal or thoracic trauma. This includes:
- Blunt abdominal trauma (motor vehicle collision, fall from height, assault)
- Penetrating thoracoabdominal trauma
- Haemodynamic instability without clear cause
- Thoracic trauma with concern for haemothorax, pneumothorax, or cardiac tamponade
FAST is not a substitute for CT in the stable patient. It is a triage tool that identifies patients who need immediate operative intervention versus those who are safe for further imaging.
The Advanced Trauma Life Support (ATLS) guidelines endorse FAST as a primary tool in haemodynamically unstable trauma assessment. A meta-analysis published in Annals of Emergency Medicine found FAST sensitivity for haemoperitoneum of approximately 79% overall, rising significantly with larger volumes of free fluid and operator experience.
Probe Selection
For the abdominal windows of FAST, use a low-frequency convex probe (2-5 MHz range). The convex provides the depth penetration needed to image the hepatorenal recess, splenorenal recess, and pelvis in most body habitus types. The Ultrascan US-CL dual-head probe switches between convex and linear modes from the same device, making it practical for the full eFAST protocol.
For the cardiac (subxiphoid) window, use the convex probe or switch to a phased array if available. The phased array footprint can be easier to angle under the xiphoid in patients with narrow subcostal windows. For the pleural views in eFAST, the linear probe is preferred for M-mode pneumothorax assessment, though the convex probe can be used.
Patient Positioning
Standard FAST is performed supine, which is usually the trauma patient's position on arrival. Free fluid accumulates in dependent spaces, so supine positioning favours fluid collection in the hepatorenal and splenorenal recesses. A small amount of Trendelenburg can improve pelvic fluid detection. Avoid rotating the patient for FAST - work around them.
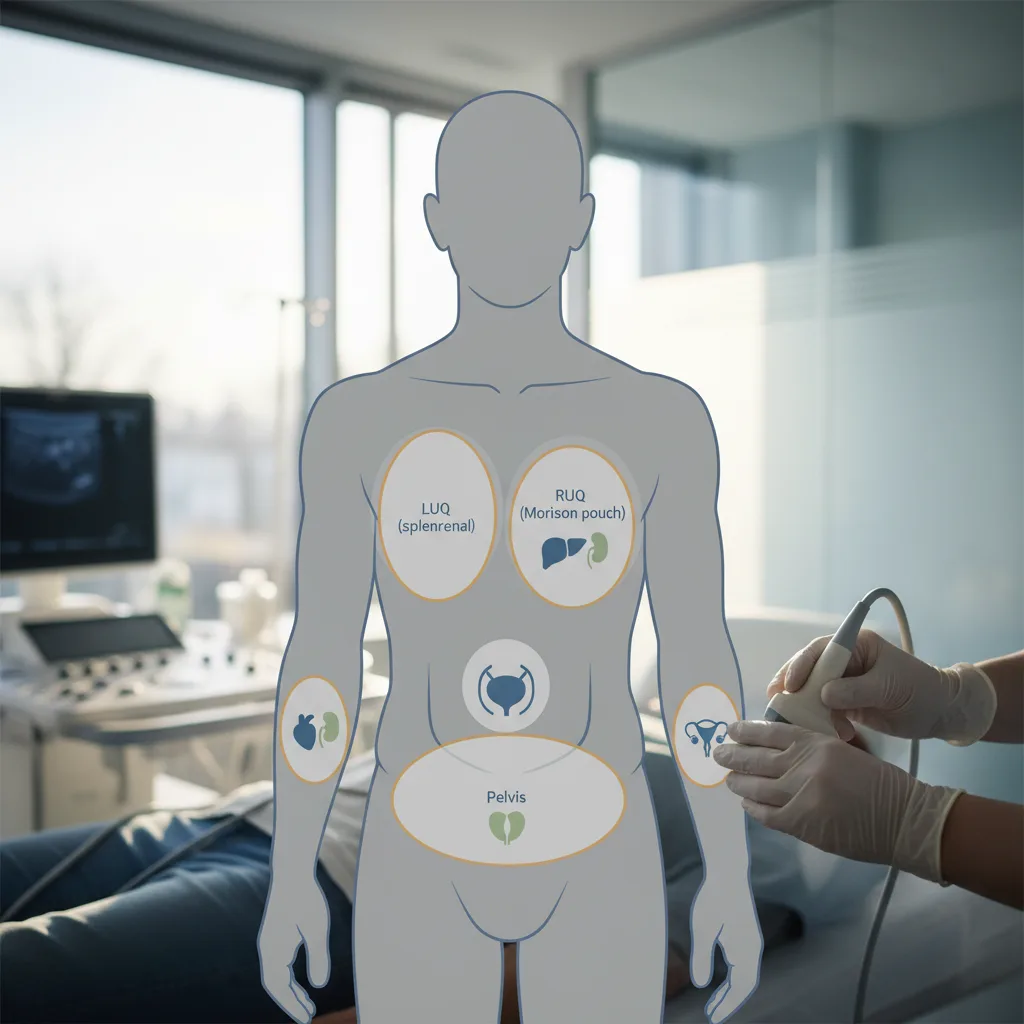
The Four FAST Windows
1. Right Upper Quadrant (Hepatorenal / Morrison's Pouch)
Place the probe in the right mid-axillary line at the level of the 9th to 11th ribs, with the indicator pointing cephalad. Angle the probe to image the interface between the right lobe of the liver and the right kidney. Free fluid appears as an anechoic (black) stripe in Morrison's pouch. Also evaluate the hepatodiaphragmatic space above the liver for a subphrenic collection.
Common pitfall: mistaking a small amount of perinephric fat (which can appear slightly hypoechoic) for fluid. True fluid is uniformly anechoic and tends to track around the organ margin.
2. Left Upper Quadrant (Splenorenal)
Place the probe in the left posterior axillary line at the 8th to 10th rib level, indicator cephalad. The left upper quadrant is more difficult to image than the right because the spleen is smaller, sits higher, and the left lung often obscures the view. Ask the patient to exhale and hold - this drops the diaphragm and improves the view. Look for anechoic fluid between the spleen and the left kidney, and in the subphrenic space above the spleen.
Common pitfall: the left upper quadrant is the most commonly missed window. Allow more time here. Stomach contents (gastric fluid) can mimic free fluid - free fluid will not be contained by the stomach wall.
3. Suprapubic (Pelvic)
Place the probe just superior to the pubic symphysis, initially transverse, then rotate to sagittal. In males, free fluid accumulates in the rectovesical pouch posterior to the bladder. In females, the pouch of Douglas (rectouterine pouch) is the most dependent pelvic space and is the first to fill with free fluid. A full bladder acts as an acoustic window - if the bladder is empty, this view is significantly compromised.
4. Subxiphoid (Cardiac)
Place the probe just below the xiphoid process, angled steeply toward the left shoulder, indicator pointing to the patient's right. Aim to visualise all four cardiac chambers in a single view. Pericardial effusion appears as an anechoic stripe surrounding the heart, typically most visible posterior to the left ventricle and anterior to the right ventricle. Tamponade physiology (right ventricular diastolic collapse) requires more experience to identify but is a critical finding.
Common pitfall: the subxiphoid view is often technically difficult in obese patients, post-operative abdomens, or patients in pain who cannot cooperate with positioning. In these cases, attempt the parasternal long-axis cardiac view as an alternative.
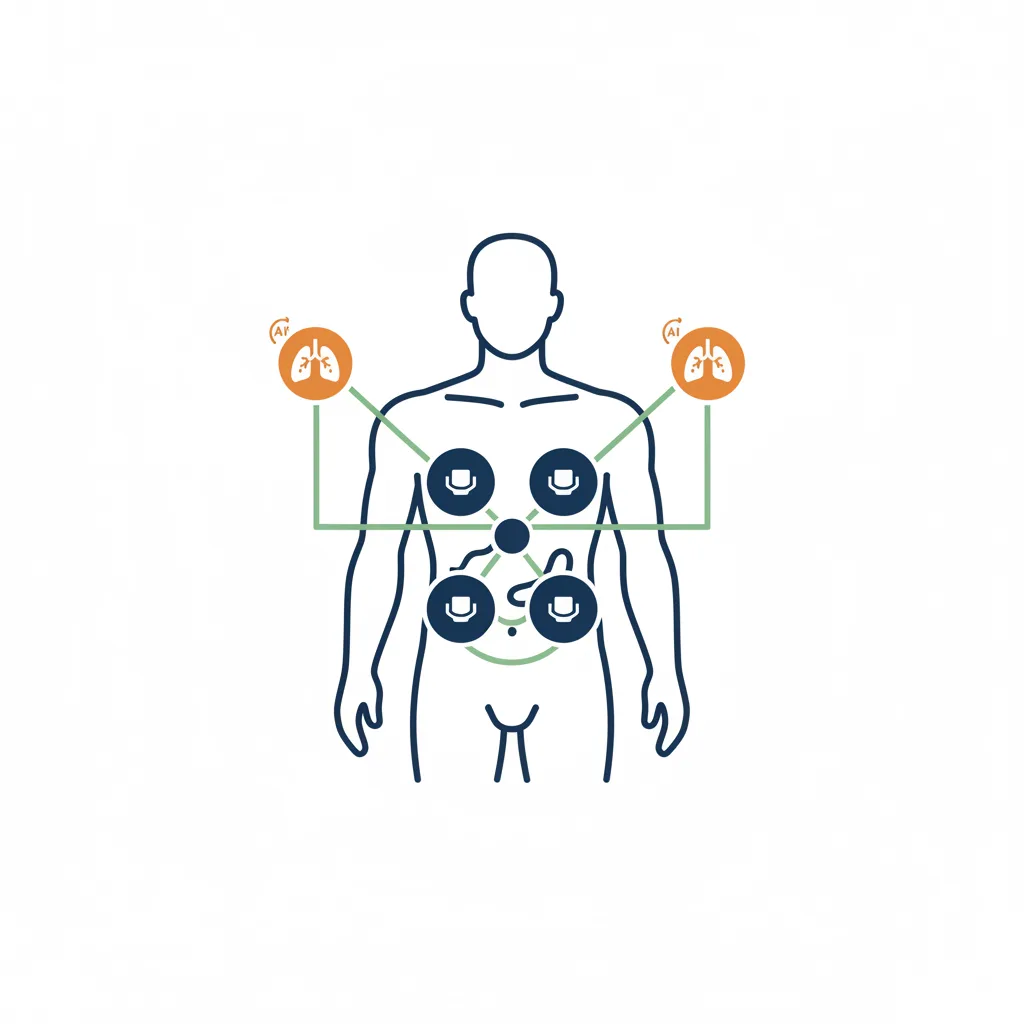
The Two eFAST Additions: Pleural Assessment
Extended FAST adds bilateral anterior chest assessment for pneumothorax. Place the linear probe in the 2nd to 3rd intercostal space, mid-clavicular line, indicator cephalad.
Normal lung: lung sliding (pleura moving with respiration) is visible as a shimmering at the pleural line. In M-mode, this produces the "seashore sign" - a wave pattern below the pleural line with a granular appearance representing moving lung tissue.
Pneumothorax: lung sliding is absent. In M-mode, the "stratosphere sign" (or barcode sign) appears - a completely linear pattern both above and below the pleural line, indicating no lung movement at that site. The absence of a lung point (the transition between sliding and non-sliding pleura) identifies the boundary of the pneumothorax.
Haemothorax in eFAST is assessed at the lateral chest in the same positions as the upper quadrant abdominal views - look for fluid above the diaphragm at the costophrenic angles.
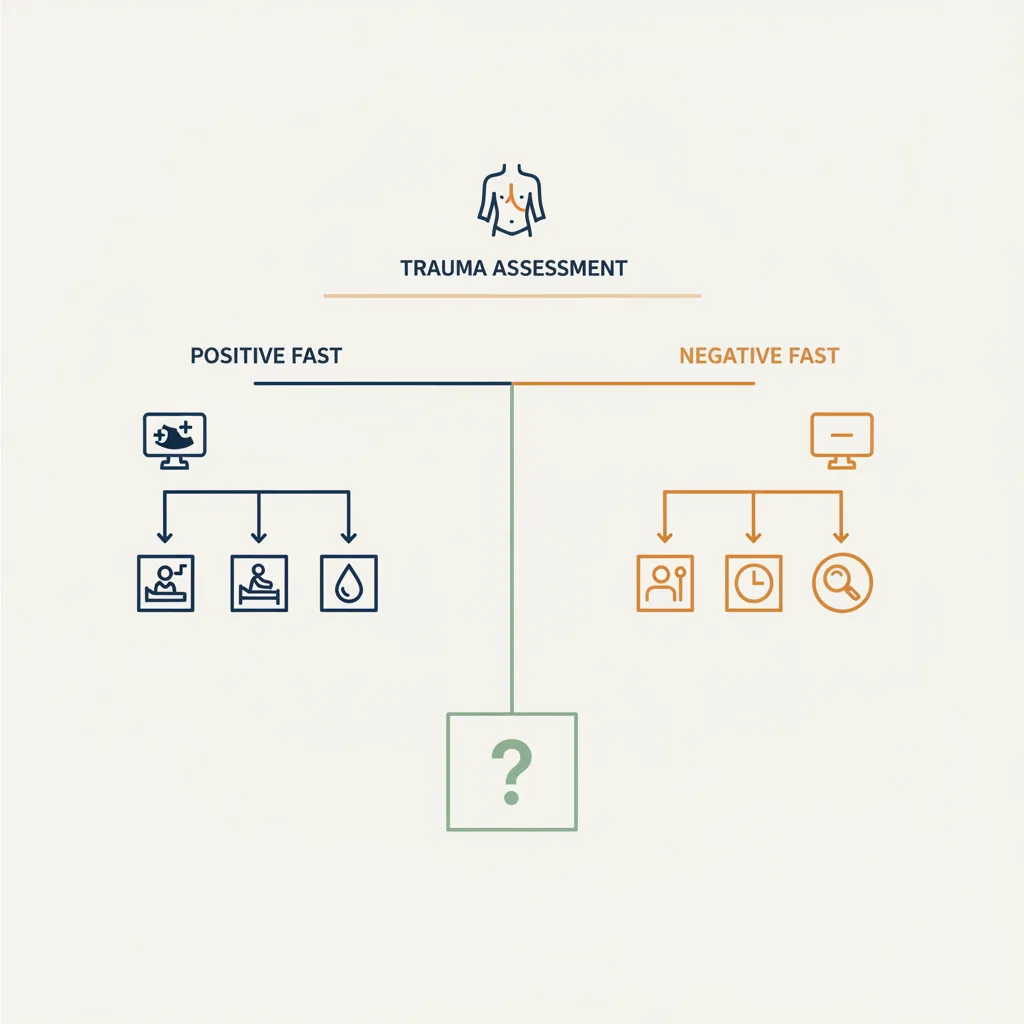
When to Escalate Beyond FAST
A positive FAST in a haemodynamically unstable patient is an indication for immediate operative intervention without waiting for CT. The question is not "where is the bleeding coming from" - it is "is this patient going to theatre now."
A negative FAST in an unstable patient does not rule out significant injury. FAST sensitivity for solid organ injury without significant haemoperitoneum is limited. A haemodynamically stable patient with a concerning mechanism and a negative FAST still warrants CT abdomen and pelvis.
For downloadable FAST protocol guides and quick-reference cards, visit the Ultrascan education resources page.
Recommended Equipment
The Ultrascan US-CL handles the full eFAST protocol with its dual convex and linear heads. For departments where cardiac imaging is a priority alongside FAST, the US-PL phased array is a strong choice. Both probes are SAHPRA-registered, require no subscription, and are supported by the South African Ultrascan team.
Visual Summary
Key concepts from this article at a glance.
Related Products
Related Articles

POCUS in Anaesthesia: Vascular, Gastric, Lung and Cardiac
A focused review of point-of-care ultrasound applications in anaesthesia practice.

Ultrasound-Guided Regional Anaesthesia: Why Visualization Matters
The case for ultrasound guidance in nerve blocks and regional anaesthesia techniques.